- 07736 104738
- sam@medicalmassagelady.com
- Mon - Sat, 8:00 - 18:30

WINGED SCAPULA/SCAPULA ALATA
When winged scapula is present, the muscles around scapula become weak or paralyzed, causing destabilisation, and this results in the medial border of the scapula protruding, like a wing, rather than resting flat against the back of the chest wall. It is often asymptomatic but may present as abnormal scapular movements with pain, weakness, or cosmetic deformity.A winged scapula can be caused by musculoskeletal or neurological issues.
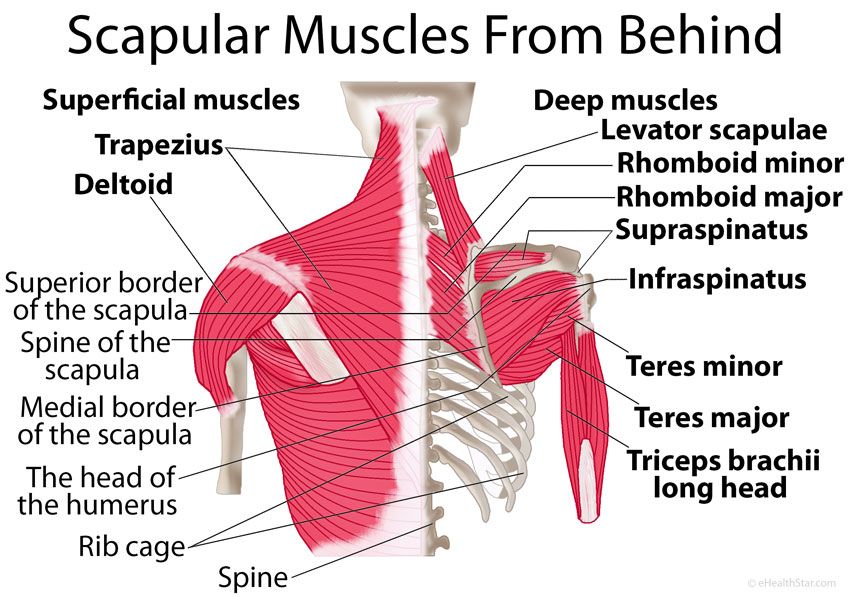
ANATOMY
The scapula is the largest bone of the shoulder and serves as an attachment point for numerous muscles which stabilise and move the arm. These muscles all work together and any dysfunction will cause arrhythmic motion of the scapula.
CAUSES
TRAUMATIC INJURY
ACUTE TRAUMA
sudden traction on the arm during a car accident or any blunt trauma to the nerves supplying the neck, shoulder and upper back, such as shoulder dislocation
REPETITIVE MICRO TRAUMAS
repeated stretching of the neck due to wearing a heavy backpack or using you arms to prop your head while lying down
NON TRAUMATIC INJURIES
- Viruses eg. influenza, polio, tonsillitis
- allergic reactions to medication
- drug overdose
- exposure to toxins,eg. herbicides
- Injections
- From birth
- post-surgical complications, eg. chest tube placement
- Idiopathic eg. congenital heart defects, cervical radiculopathy, and muscular dystrophy,
- Parsonage-Turner Syndrome
SURGICAL
- some surgeries may cause nerve damage eg
- .rib resections,
- mastectomies
- 8% of axillary dissection cases demonstrate scapular winging 15 days post surgery
- procedures that require general anaesthesia
A winged scapula is usually caused by nerve damage on one of the following 3 nerves which control arm, back, and neck muscles:-
- the long thoracic nerve, which controls the serratus anterior muscle
- the dorsal scapular nerve, which controls the rhomboid muscles
- the spinal accessory nerve, which controls the trapezius muscle
This nerve damage can be a result of injury or surgery.
Muscular dysfunction can also be the cause.
MUSCULAR DYSFUNCTION VERSUS NERVE DYSFUNCTION
MUSCULAR DYSFUNCTION
The following muscles may be involved:-
- Trapezius
- serratus anterior
- rhomboids
- levator scapulae
- pectoralis minor
- latissimus dorsi
NERVE DYSFUNCTION
The following nerves may be involved:-
- accessory nerve
- long thoracic nerve
- brachial plexus
Damage to these structures may lead to:-
LOSS OF SERRATUS ANTERIOR MUSCLE FUNCTION
The serratus anterior muscle attaches to the medial anterior aspect of the scapula, anchoring it to the rib cage.
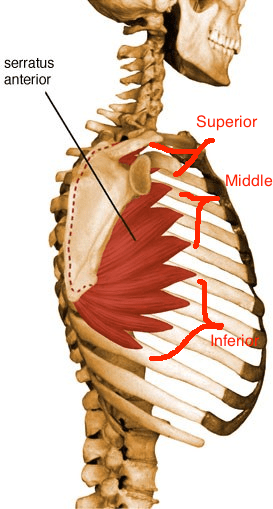
True winging is not common, and is usually a result of traumatic injury or inflammation of the long thoracic nerve, running from the neck to the serratus anterior muscle. The position of this nerve makes it more vulnerable to injury.
A winged scapula due to long thoracic nerve injury can be identified by asking the client to push against a wall from about 2ft away, with flat palms at waist level.

The nerve can be decompressed at the scalene muscles in the neck.
LOSS OF TRAPEZIUS MUSCLE FUNCTION
The trapezius lifts and rotates the scapula, helping to shrug your shoulders. Isolated loss of trapezius function is rare, sometimes resulting from radical neck surgery on tumours where the accessory nerve may be damaged. The shoulder will be depressed and the scapula translated laterally, with the inferior angle rotated laterally.

When there is trapezius weakness due to accessory nerve damage, a client will be unable to lift arm off the couch in supine position or have difficulty with overhead activities. Surgical reconstruction or nerve release may be possible treatments.
WEAKNESS OF THE SCAPULA STABILISERS
Fascioscapulohumeral dystrophy (FSHD), a form of muscular dystrophy, is the main cause of weakness in the stabilising muscles (ie. serratus anterior, trapezius, rhomboids and latissimus dorsi).

Other noticeable characteristics will include:-
- The scapula rising into the trapezius
- Hypertrophied deltoids
- Profound winging of the medial border of the scapula
- There may also be some facial weakness
LOSS OF THE SCAPULAR SENSORY MECHANISM
The clavicle and scapula are connected by the coracoclavicular ligaments.
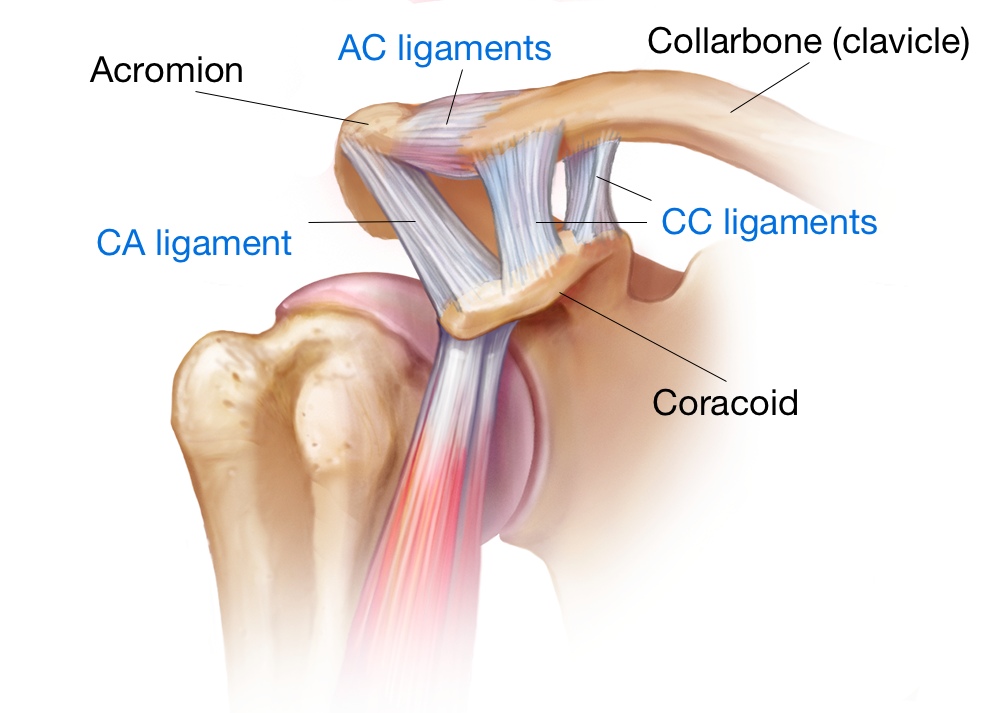
The scapula is connected to the rest of the body by the acromioclavicular joint, so
- a lateral clavicular fracture
- an acromioclavicular dislocation
- ruptured coracoclavicular ligaments
- scapulothoracic dissociation
will destabilise the shoulder joint, causing scapula winging with overhead movement.
SECONDARY WINGING DUE TO INSTABILITY
Scapula winging and dysrhythmia commonly result from instability caused by recurrent shoulder dislocations. This leads to muscle dysfunction which is worse with more frequent and less traumatic dislocations.
SECONDARY WINGING DUE TO PAIN

Painful shoulder conditions and reduced range of motion in the glenohumeral joint cause us to compensate with abnormal movements of the entire shoulder complex
BRACHIAL PLEXUS INJURY

The stabilising muscles of the shoulder are mostly controlled by the brachial plexus, a bundle of nerves running from the neck to the arm. Conditions such as brachial neuritis (Parsonage- Turner syndrome) can lead to weakness of the scapula muscles due to the nerves being inflamed.
SYMPTOMS
- severe pain which often disturbs sleep – usually in winged scapula caused by nerve trauma
- no pain – if caused by muscular trauma
- a shoulder blade that sticks out - can make sitting and wearing a backpack uncomfortable
- weakened neck, shoulder and arm muscles – due to nerve trauma
- may be difficulty in raising your arm above the shoulder.discomfort in your neck, shoulders, and back
- fatigue
- a drooping shoulder

- cervicogenic headaches – originate in the upper cervical spine, referring pain to the head. There may also be referred pain from the upper trapezius or trigger points in the sternocleidomastoid
TYPES OF MUSCULAR SCAPULAR DEVIATION
TYPE 1

- a visible inferior anglea pronounced anterior tilt of the scapula
- shortening of the pectoralis minor
- shortening of the posterior joint-capsule
- muscular imbalance of the lower, ascending section of the trapezius and the serratus anterior
TYPE 2

- a visible margo medialis
- internal rotation of scapula
- shortening of the posterior joint-capsule
- shortening of the latissimus dorsi
- muscular imbalance of the trapezius and serratus anterior
TYPE 3
- a visible inferior angle
- downward rotation of scapula
- shortening of the levator scapulae
- muscular imbalance of the upper and lower trapezius (pars descendens and ascendens)

TYPES OF NEUROLOGICAL SCAPULAR DEVIATION
TYPE 1
- a separated scapula from the thorax
- elevated scapula
- margo medialis is nearer the spinal line
- damage of the long thoracic nerve
- dysfunction of the serratus anterior
TYPE 2
- a separated scapula from the thorax
- lowering of the scapula
- damage to the accessory nerve
- dysfunction of the upper trapezius (pars descendens)
PREVENTION
Scapular winging may not be preventable in every case, but the risk can be reduced by:-
- avoiding repetitive shoulder/arm movements
- maintaining correct posture
- using an ergonomic chair or pillow
- using shoulder-friendly ergonomic backpacks
- avoiding carrying excess weight on your shoulders
- stretching and strengthening the neck/shoulder/arm muscles
TREATMENT
Treatment may be surgical or non surgical, depending on the cause, but medical management may be more appropriate in older people with a sedentary lifestyle or minimal symptoms.
SURGICAL
Surgery is more likely when non surgical methods have not worked, in cases of traumatic injury or where there has been spinal accessory nerve damage.
- SPLIT PECTORALIS MAJOR TRANSFER
Part of the muscle (or sometimes nerve) is relocated to the back or shoulder
- MODIFIED EDEN-LANGE PROCEDURE
( Eden Lange involves lateral transfer of the levator scapulae, rhomboid major, and rhomboid minor to reproduce the functions of the trapezius and support the scapula, in cases of nerve paralysis)
The modified procedure transfers the rhomboid minor insertion to the supraspinatus fossa, compensating for the mid trapezius and stabilising the superior angle of the scapula.
- SCAPULOPEXY/STATIC STABILISATION
The scapula is attached to a rib or vertebra. This may result in bone fractures, lung problems and inability to lift the arm, hence is a last resort.
NON SURGICAL
scapular winging due to serratus anterior damage may heal within 2 years without any treatment
- anti-inflammatories
- muscle relaxants
- analgesics
- physiotherapy
- using a brace for several months in the early recovery period
- physiotherapy and massage for dorsal scapular nerve damage
- home exercises
RECOVERY
Recovery can take several months to years, but certainly early treatment will improve the outcome, depending on:-
- the severity of the damage
- whether the person undergoes surgery
- which nerves or muscles are damaged
EXERCISES
Stretching exercises may help strengthen and improve range of motion, but can sometimes make the problem worse.
SCAPULAR RETRACTION
- pull the shoulder blades back while in a standing position, holding for 10 seconds. Rest for10 seconds, and repeat 10 times.

EXTERNAL ROTATION
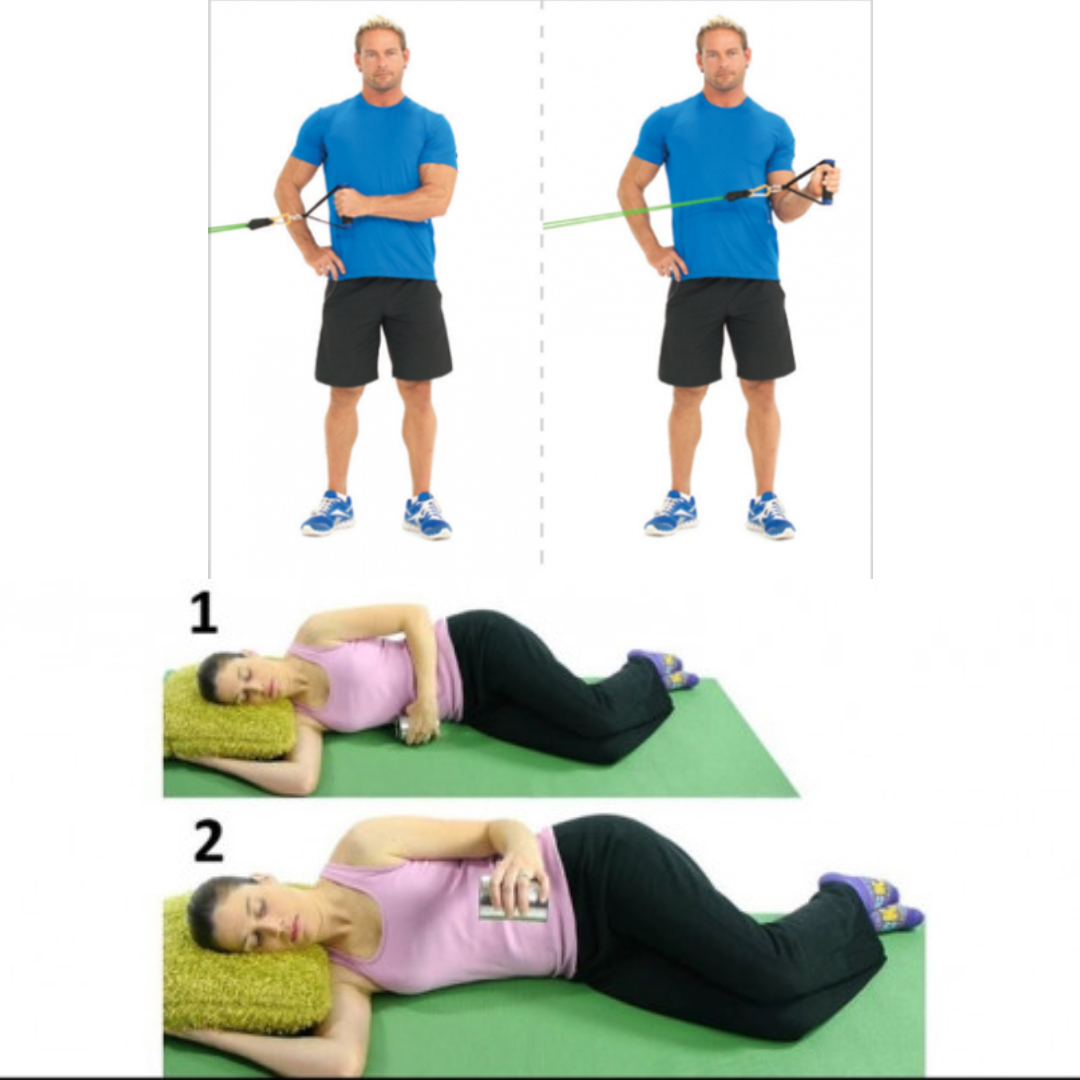
– can be done with a resistance band or light dumbbellAttach an exercise band to a closed door , holding it with a hand crossed over the body, elbow at 90 degrees, then pull the band in front of the body and to the side, not moving the elbow. Repeat this 12–15 times. Alternatively do in a side lying position if using a dumbbell.
STANDARD PUSHUPS


- The back should be flat, the legs should be outstretched, and the hands should be flat against the floor, farther apart than the width of the shoulders. Bend the elbows and lower the body to the floor. Then, push the body up, resuming the starting position. Slowly increase reps up to 12–15.
PLANKS WITH SHOULDER TAPS
BEAR CRAWLS


